How to Fix Scapular Winging
Jun 17, 2022
Introduction:
What do you automatically think of when you hear the words scapular winging?
Do you think serratus anterior weakness?
Do you think long thoracic nerve dysfunction?
Do you think tight scapular muscles?
While these thoughts are most likely contributing factors, I believe they're premature. Instead, they are the symptoms of the actual problem and become easy to blame and disguise the source of the true dysfunction. In this article, I'll discuss the following topics:
- Scapular Winging Overview
- Scapular Biomechanics
- Posturally Driven Scapular Winging
- Respiration Reaching Drills
- Strengthening Exercises
If you're a visual learner, click the video below to learn these same concepts.
Scapular Winging Overview:
Before discussing this redefined approach to fixing scapular winging, we first must understand the traditional thought process.
Scapular winging is a common dysfunction when the scapula's medial border "wings" off the rib cage. The area that is winging usually isn't painful, and most people have a degree of scapular winging without any symptoms. However, it can contribute to limited or dysfunctional shoulder movement in other situations. The most common traditional explanations for this winged position are serratus anterior weakness, long thoracic nerve dysfunction, and tight scapular muscles.

The serratus anterior is usually the main suspect because its main action is to protract and upwardly rotate the scapula. Additionally, when it's appropriately contracted, its function is to remain congruent with the rib cage. So, you can understand when there's a visual positional disturbance such as scapular winging; the serratus anterior is an easy go-to muscle to blame.

But... what if the scapula didn't move away, but the rib cage did?
Scapular Biomechanics:
To better understand the response of a posturally-driven scapular winging, let's briefly discuss scapular biomechanics.
Most of us can visualize what upward rotation, downward rotation, protraction, and retraction looks like. However, can you do it if I tell you to imagine internal or external rotation quickly? These two motions play a significant role in scapular winging but are often forgotten.
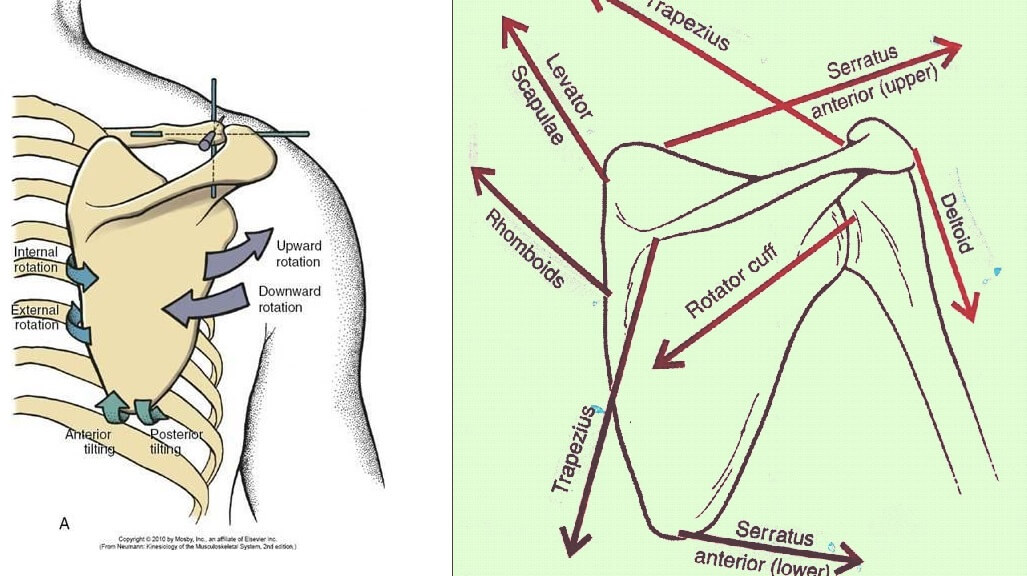
The easiest way to remember internal and external rotation is if you think about a gate or a door. External rotation represents a gate/door that is closed. This is desired when the shoulder protracts in combination with the serratus anterior contraction.
 Conversely, internal rotation represents an open gate/door and scapular winging. How much the door is open can be synonymous with the varying degrees of scapular winging.
Conversely, internal rotation represents an open gate/door and scapular winging. How much the door is open can be synonymous with the varying degrees of scapular winging.

Posturally Driven Scapular Winging:
It's no secret that most, if not all, of our patients, don't have "perfect" upright posture. Although, I would agree that that's a good thing. I believe that the best posture is the variable one. Meaning that too much flexion is bad and too much extension is bad. The ideal posture needs to ebb and flow to remain pain-free.
However, there are postural commonalities due to the asymmetries of the human body. We won't get into all the specifics in this article, but these asymmetries produce postural patterns. A typical posture is a right shoulder lower than the left, a thorax collapsed forwards, and a thorax rotating to the right.
Why is this important to scapular winging, you may be asking? Well, there's a direct consequence at the scapula from this posture! Your brain doesn't like being in this forward collapsed position, so it will try to move out of it. Usually, the spine is too stiff to create a new pattern, so the brain goes to a more mobile target — the humerus. In an attempt to upright the spine, the humerus moves into a more externally rotated position. As a result, the scapula moves into internal rotation — the "doors" are now open, and you now have a winging scapula.
If you have difficulty visualizing this, check the associated video to see this postural demonstration.
Respiration Reaching Drills:
Breathing is usually the most neglected intervention in scapular winging dysfunction. However, it can be powerful when utilized in conjunction with the proper serratus anterior contraction.
Remember how we talked about the forward and rotated posture? This tends to compress the right anterior chest wall, making it difficult to expand. So, we can utilize inhalation with reaching exercises to help expand this overall compressed area.
The key to reaching is that you need to find the sweet spot. I suggest placing your client in a quadruped position and having them find their 25%, 50%, 75%, and 100% protaction. This is highly beneficial for them to learn, so they know how much is "enough."
The correct method is to "close" the gates and increase congruency. You'll most likely have your patient below 50% of their max protraction to achieve this.
The incorrect technique is over rounding through maximal protraction. This will bias more of an IR, open gate position of the scapula. This will be counterproductive to your intent.
View this post on Instagram
Strengthening Exercises:
Once you've achieved increased scapulothoracic congruency and a better position, it's time to strengthen. You've already worked on the serratus anterior with your reaching drills, so what's next?
The low trap and the long head of the triceps.
The low trap is usually a familiar go-to muscle, but the long head of the triceps is not as expected. Remember, this muscle attaches directly to the scapula and will influence upward rotation/posterior tilt.
Check out the following three exercises that seek to address the following:
- Expand and move the thorax back
- Address postural asymmetries (right rotation)
- Strengthen the serratus anterior, low trap, and long head of the triceps
Conclusion:
As you may have noticed, this approach isn't that much different than the traditional! The only difference I want you to implement is increasing your awareness and ensuring that the scapula is in a good starting position before strengthening. To do that, we look at the ribcage first and then the scapula. If you can achieve this, you'll produce better long-term solutions for your patient.
Enjoy learning practical topics like this one? Join The PR Club for Free to gain instant access to 100+ educational movement videos just like this!